
Corneal ectatic disorders, such as keratoconus, progressively weaken corneal integrity, leading to thinning, irregular astigmatism and visual deterioration.1 Typically progressive in nature, these ectasias result in increasingly thinner corneas, causing the cornea to protrude forward into a cone shape. This leads to increasing amounts of myopia and astigmatism – both regular and irregular – as the disease progresses, significantly degrading visual acuity, visual quality and overall quality of life.
Historically, management strategies have included rigid contact lenses and corneal transplantation, both of which primarily address symptoms rather than halting disease progression. Corneal cross-linking (CXL) has emerged as an effective intervention to stabilize the cornea by strengthening collagen fibres, effectively halting disease progression.2 However, traditional, non-customized CXL methods achieve little in terms of cone flattening and visual rehabilitation.2
The introduction of intracorneal ring segments (ICRS) in 1993 revolutionized treatment by mechanically reshaping the cornea to improve visual acuity.3 However, synthetic polymethylmethacrylate (PMMA) ICRS, while effective in regularizing corneal topography, also present significant drawbacks, including extrusion, stromal melt, neovascularization and non-physiological stress on corneal tissue.4–11 Additionally, their rigidity limits adaptability in advanced cases with irregular topography or thinner corneas.
The evolution of CAIRS
Soosan Jacob proposed corneal allogenic intrastromal ring segments (CAIRS) in 2018 to overcome limitations, utilizing donor corneal tissue to improve biocompatibility and integration.12 CAIRS demonstrated reduced risks of extrusion and necrosis compared with synthetic alternatives.12,13
Interestingly, Asfar et al. demonstrated that CAIRS outperform synthetic ICRS in improving corrected distance visual acuity, topographic astigmatism, keratometry and vertical coma, with 60% of CAIRS-treated eyes gaining two or more Snellen lines compared with 31.58% in the ICRS group.13
More recently, further advancements were made. One was the development of femtosecond laser-assisted CAIRS (femto-CAIRS), which improved precision by creating highly accurate intrastromal tunnels and rings.14 This innovation increased the technique’s reproducibility and allowed for customized segment placement.
However, the inherent pliability of allogenic tissue posed challenges during insertion, requiring novel approaches to facilitate handling. Techniques such as air-drying the ring segments (the ‘Jerky Technique’) provided only temporary rigidity due to rehydration upon contact with the patient’s cornea during implantation, rendering its placement more complicated than in the initial stages of this part of the procedure.15,16
ECO-CAIRS: enhancing the corneal ring’s stiffness
Despite the advancements offered by CAIRS (assisted or not by femtosecond laser), challenges related to the pliability of allogenic tissue persisted, hindering surgical handling and placement consistency. In response, extracorporeal cross-linking-optimized CAIRS (ECO-CAIRS) was introduced to enhance segment rigidity, simplifying the insertion process and improving surgical outcomes.17
ECO-CAIRS involves the application of ultra-high-fluence CXL (up to 30 J/cm²) to donor corneal segments prior to implantation (Figure 1A). This process effectively stiffens the allogenic tissue, ensuring that it remains rigid throughout insertion and the perioperative period.17,18 Unlike dehydration techniques, which offer only temporary stiffness, the cross-linking procedure provides sustained structural integrity, facilitating more predictable placement and reducing the learning curve for surgeons, even if the ring segment becomes hydrated during the procedure.15–17 Except for the extracorporeal cross-linking of the allogenic ring segments, the procedure adheres entirely to the standard femto-CAIRS protocol.14,17
Figure 1: The ECO-CAIRS segment: preparation and post insertion
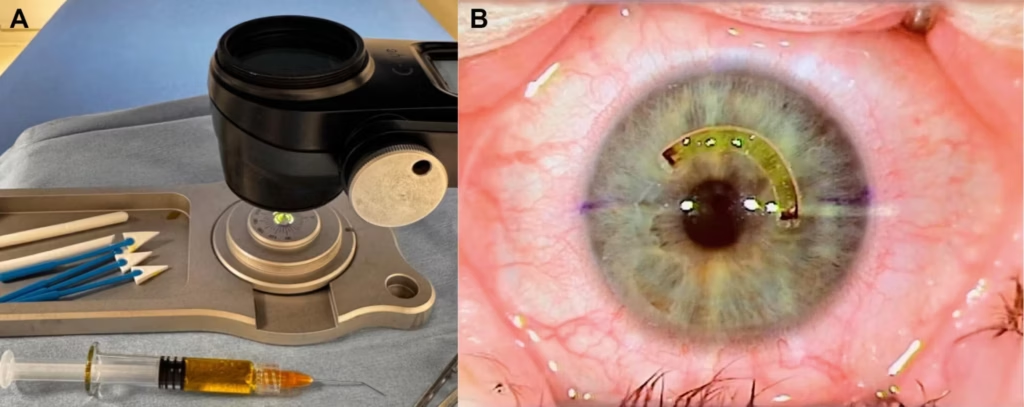
A: Riboflavin-soaked corneal allogenic ring segment undergoing extracorporeal high-fluence corneal cross-linking. B: Extracorporeal cross-linking-optimized corneal allogenic intrastromal ring segment ring piece, in situ, just after implantation. The yellow colour fades over the following days and weeks
Biomechanically, ECO-CAIRS offers several advantages. The cross-linked segments resist rehydration-induced softening, allowing for an easier and more precise positioning within the femtosecond laser-created intrastromal tunnel. Additionally, the process results in a temporary reduction in segment thickness, enabling the insertion of greater segment volume within the corneal stroma, which might enhance the overall flattening effect and topographic improvement.18
Most importantly, the high ultraviolet (UV) fluence cross-linking protocol not only eliminates all keratocytes within the segment but also kills all potential micro-organisms on the segment’s surface.17 This mechanism should reduce the risk of infection and the risk of keratocyte-mediated rejection, making the segment similar to the gamma-sterilized industrial segments provided by commercial entities.11,17
With respect to surgical planning, current ECO-CAIRS implantation follows the established femtosecond-assisted CAIRS nomogram described by Bteich et al.14 In the initial ECO-CAIRS clinical study, allogenic ring segments with arc lengths of 140–160° and widths of 800–825 µm were implanted into femtosecond laser-created intrastromal tunnels of 170–200°.17 The development of a dedicated ECO-CAIRS-specific nomogram is currently under way, and several parameters are under consideration, including cone location, pachymetry in both the cone and peripheral regions and other factors identified by clinically usable corneal biomechanical assessments.17
In the published ECO-CAIRS clinical series, the increased stiffness of the segments simplified insertion and reduced operative time.17 After the surgery, as expected, optical coherence tomography (OCT) imaging reveals stable integration of the segments with the surrounding cornea (Figure 2). Similarly, the yellow colouration of the ring segment, which had been soaked in riboflavin (Figure 1B), becomes imperceptible over the days and weeks following the surgery. Furthermore, the high-fluence cross-linking eliminates viable keratocytes within the donor tissue, reducing the potential risk of keratocyte transmission from donor to recipient.17,18 The extent to which this factor has an immediate or long-term clinical impact remains to be determined. Future research aims to further optimize the treatment protocol by investigating the long-term biomechanical effects and refining surgical nomograms to enhance visual rehabilitation outcomes.
Figure 2: Corneal OCT of the implanted ECO-CAIRS segment at 1-month and 1-year post-implantation
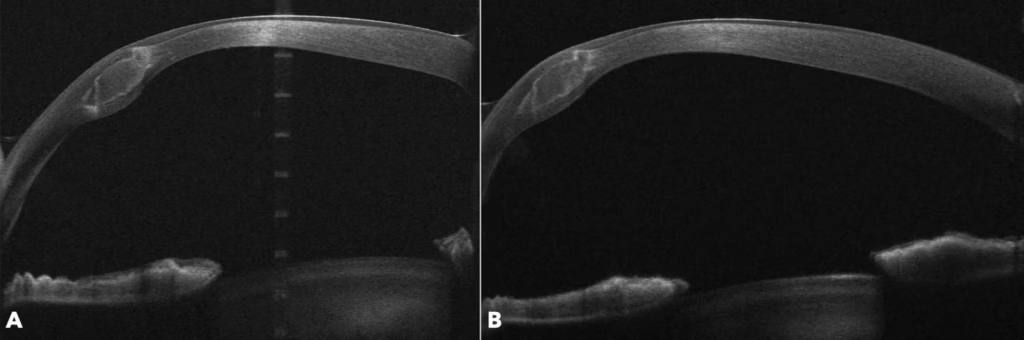
Corneal optical coherence tomography images of the same (right) eye after extracorporeal cross-linking-optimized corneal allogenic intrastromal ring segment transplantation (250°–70° section) showing tissue integration and stromal and epithelial remodelling
A: Image at 1 month. B: 1 year postoperatively. At both time points, no evidence of extrusion or oedema is visible
In the published ECO-CAIRS clinical series, implantation was uneventful in all cases, with the cross-linked allogenic segments remaining stiff throughout the entire insertion and positioning process and showing no tendency to soften during handling.17 High-resolution anterior segment OCT demonstrated a marked but transient reduction in segment thickness immediately following extracorporeal cross-linking, with representative measurements showing thinning from approximately 650 µm pre-CXL to 252 µm immediately post-CXL. Progressive rehydration was observed over the first postoperative days, with thickness increasing to approximately 312 µm on day 1 and 354 µm on day 2. Early postoperative corneal topography demonstrated localized flattening effects consistent with the intended biomechanical action of the implanted segment, although the study was not designed to assess refractive or keratometric outcomes.17
Biomechanical assessment using OCT elastography
It would not be surprising to expect that a rigid synthetic ring might exhibit biomechanical behaviour different from that of a flexible allogenic material such as a cornea. Interestingly, this remains an area of study that has received little attention to date.
So far, the nomograms we use for rigid PMMA ring segment implantation in keratoconus are primarily based on corneal topography or shape and the patient’s refraction, considering the rigid nature of the implanted PMMA material. While there have been suggestions to develop nomograms that account for flexibility similar to that of human corneal tissue used in CAIRS, this aspect is still under investigation.
Our group has previously demonstrated, through a series of published studies utilizing OCT elastography, the biomechanical behaviour of corneal tissue surrounding a synthetic ring implant.19–21 In other words, we observed that ICRS induces localized strain patterns, which vary with the arc length of the implanted ring.
The same question arises regarding the biomechanical impact when more flexible rings or tissues are used. In this context, our group conducted preliminary, unpublished studies that demonstrated a distinct biomechanical behaviour compared with the synthetic rings previously discussed. Preliminary data presented at the European Society of Cataract & Refractive Surgeons (ESCRS) 2024 conference in Barcelona indicated no significant change in corneal strain around the implanted CAIRS segments, suggesting a potentially meaningful difference, although work on this topic is currently on-going.22 We are currently conducting biomechanical studies using OCT elastography to further explore this, with results expected in the coming months.
Integration with other procedures
CAIRS, including the advanced ECO-CAIRS technique, holds significant potential when integrated with other established procedures for vision rehabilitation in corneal ectasias.12,17 Furthermore, combining CAIRS with complementary interventions (like therapeutic excimer laser phototherapeutic keratectomy in suitable corneas to reduce higher order aberrations) may help further optimize visual outcomes.12
One of the most frequently employed combinations is CAIRS with CXL. While CAIRS provides mechanical reshaping of the cornea, CXL enhances corneal biomechanical stability by strengthening stromal collagen and proteoglycan bonds, and we have developed an approach called ELZA-PACE (phototherapeutic keratectomy [PTK]-assisted customized epithelium- (epi-)on CXL), which uses the excimer laser to solely remove epithelial tissue over the cone (no stroma) to generate an epi-on/epi-off hybrid cross-linking procedure. Differential UV fluence delivery to the cone and the non-cone regions of the cornea then results in a strong (>10 D) flattening effect. This synergistic approach can therefore stabilize ectasia (the CXL component) while improving corneal regularity, further enhancing visual outcomes. The timing of these procedures – whether performed simultaneously or in a staged approach – remains an area of active investigation.
Finally, in cases where refractive errors persist beyond the capabilities of corneal interventions, CAIRS can be potentially combined with lens-based solutions such as phakic intraocular lenses. This combined approach offers a viable option for patients with advanced keratoconus, providing enhanced visual rehabilitation while maintaining corneal structural integrity.
Alternative approaches
Other allogenic stromal augmentation approaches have been evaluated as methods for rehabilitating the shape of ectatic corneas. These include stromal lenticule addition keratoplasty and related techniques, which involve the implantation of a negative meniscus-shaped human donor lenticule (or a more customized shape) at a depth of ~120 µm.23,24 Lenticules obtained from myopic Kerato-lenticule Extraction (KLeX) surgeries have also been used in this manner.25 A xenogenic approach, in which acellular porcine collagen implants are used as an alternative to human donor cornea/KLeX tissue, has also been used clinically.26,27
Conclusion
CAIRS and their evolution into the femtosecond- and extracorporeal cross-linking-optimized-CAIRS represent a worthwhile advancement in the management of corneal ectasia.12 These techniques offer a promising alternative to synthetic ICRS, providing improved biocompatibility, better integration with host tissue and reduced complication rates, such as infection and rejection.
ECO-CAIRS addresses challenges associated with conventional CAIRS procedures by enhancing segment rigidity through ultra-high-fluence CXL prior to implantation.17,18 This innovation simplifies the insertion process, improves surgical reproducibility and reduces the learning curve for surgeons. Furthermore, the temporary thinning effect induced by the cross-linking process may allow for the implantation of greater segment volumes, potentially enhancing corneal flattening and topographic outcomes. When integrated with complementary procedures, such as CXL and excimer laser treatments, CAIRS and ECO-CAIRS offer a comprehensive approach to keratoconus management.12,17
Despite these promising outcomes, further research is required to optimize treatment protocols, refine patient selection criteria and evaluate the long-term biomechanical effects of CAIRS and ECO-CAIRS. Future studies should also explore the potential of personalized treatment plans based on corneal topographic and biomechanical characteristics to maximize visual and structural benefits.












