
Conjunctival nevi are common benign lesions of the conjunctiva. Occasionally, they can transform into, or be confused with, aggressive malignancies such as melanomas. They can present at any age, including in children and adolescents. While usually asymptomatic, they can cause psychological discomfort, irrespective of the size or severity of the lesion.1 Nevi can be a concern as being malignant for patients or the healthcare provider, cause ocular surface irritation or become a cosmetic anomaly. Occasionally, they can be inflamed and cause pain.2 Conjunctival nevi are usually managed by carefully monitoring the lesion for a change in appearance. In other cases, they are treated by laser or surgical removal. In a series of 255 cases of conjunctival nevi, the most common indications for surgical removal were documented tumour growth, limbal location with involvement of the cornea and the presence of prominent feeder vessels.3 Removal of the nevus can be accomplished by either argon laser photoablation or surgical excision of the tumour.1–6 This article provides our experience in managing conjunctival nevi and is also a concise review of the condition, focusing on their laser and surgical treatments.
Methods
This prospective study was conducted in accordance with the principles outlined in the Declaration of Helsinki of 1964 and its later amendments. The Institutional Review Board permission was obtained for this study (certificate no. AEC_01_CN). Written consent for the procedures was obtained from all patients. The study involved 40 patients identified to have a benign conjunctival nevus. There were no patients with multiple or bilateral nevi.
The study was conducted between January 2024 and January 2025. It involved 28 male and 12 female patients. The choice of treatment was decided by observing the site, size and presumed depth of the lesion on slit-lamp examination and by discussing the choice of treatment with the patients. The patients underwent argon laser photoablation (n=32) or surgical excision (n=8) of the nevus and were followed up for at least 3 months. All patients had a 100% success rate in terms of complete removal of the conjunctival nevus and the absence of any complications such as neovascularization, haemorrhage, scarring, recurrence or infection.
Conjunctival nevi
Conjunctival nevi (also known as eye freckles) are the most common benign tumours of the conjunctiva, comprising nearly 17.2–42% of all conjunctival tumours.7,8 These tumours are more commonly found in white individuals and typically appear and enlarge between the first and early third decades of life, with an equal distribution between men and women.7,9–11 In a study of 410 patients with conjunctival nevi reported by Shields et al., the mean age at initial presentation was 32 years.2
Epibulbar melanocytic lesions can involve the conjunctival epithelium, stroma and sclera. Such lesions include nevi, conjunctival racial melanosis, primary acquired melanosis (PAM), secondary melanosis, melanoma, ocular melanocytosis and extraocular extension of uveal melanoma.2
Conjunctival tumours range from various benign conditions, such as limbal dermoid or myxoma, to malignant and potentially life-threatening tumours, including melanoma or Kaposi’s sarcoma.2
Benign conjunctival lesions of melanocytic origin are divided into two broad categories: nevi and other benign disorders such as complexion-associated pigmentation, pigmentation associated with systemic disorders, ephelis and lentigo. Nevi are subdivided according to the age of first clinical presentation: congenital (present at birth or appearing within the first 6 months of life) or acquired. Acquired nevi usually become clinically apparent during the first or second decade of life. They appear as a discrete, somewhat elevated, sessile lesion that can be variably pigmented, may show characteristic clear intralesional cysts and is commonly situated in the interpalpebral conjunctiva. The presence of dilated feeder vessels or episcleral vessels is unusual.3,10
Conjunctival nevi typically appear in children and young adults as lightly pigmented or amelanotic, flat or raised nodules, which often show accelerated growth during puberty or pregnancy.8 According to Shields and Shields, in 5% of cases, the lesions become more or less pigmented over time and show enlargement in 7% of juvenile patients.12
Conjunctival nevi are classified into two categories based on their clinical manifestations: superficial nevi and deep-vascularized nevi. Superficial conjunctival nevi exist in the conjunctival stroma. They are typically flat, brownish or tan in colour, occasionally amelanotic, without connections to surrounding vessels, are free to move over Tenon’s capsule or the sclera and do not contain a cyst. On the other hand, a deep-vascularized nevus is elevated, can contain a cyst and has feeder vessels that originate from the conjunctiva.6
Histologically, conjunctival nevi are similar to cutaneous nevi. However, since the conjunctiva is devoid of the dermis, the terms subepithelial and stromal are used instead of dermal.
The nevi are histologically classified into the following types, based on the location of the melanocytes:
-
Compound: Compound nevi comprise 70–78% of all conjunctival nevi and are the most common type. They are characterized by nevus cells in the epithelial–subepithelial junction and the subepithelial stroma. They also have epithelial intrusions into the lamina propria and intralesional epithelial cysts lined by conjunctival epithelium and goblet cells. The cysts are present in 50% of the cases. The cysts increase with time, rarely occupying the entire lesion, so that the melanocytic component may not be evident.
-
Subepithelial: These nevi are characterized by lesions confined to the subepithelial region. They are present in 9% of all cases and usually occur in older patients.
-
Junctional: Nearly 5% of all conjunctival nevi are of the junctional type. They are usually seen in younger age groups. They have characteristic nested, but occasionally lentiginous proliferations of type A or B cells situated at the epithelial–subepithelial junction. Junctional nevi are regarded as an early stage in the evolution of compound nevi.
-
Juvenile conjunctival nevus: These nevi are histologically characterized by a confluent growth pattern in the junctional component and a paradoxical reverse maturation pattern, which shows the nuclear and cytoplasmic size of melanocytes in the subepithelial region being greater than that seen in the junctional component. In some cases, a prominent inflammatory reaction is present, obscuring the architecture of the nevus and causing a misleading impression of cytological atypia.7,10
Several variants of nevi have been reported.7 These include combined nevus, balloon cell nevus, Spitz nevus, pigmented spindle cell nevus and blue nevus.
The differential diagnosis of conjunctival nevus includes other non-pigmented conditions such as conjunctival cysts, inflamed pinguecula, allergic conjunctivitis, episcleritis, foreign body granuloma, squamous epithelial neoplasia or lymphangioma, and pigment deposits from silver and iron.2,13
Nevi are ostensibly common in individuals with brown irides.2 Nevi were seen in 55% of patients with brown irides in Shields et al.’s study and 78% of patients (60/77) in a survey from the Moorfields Ocular Oncology Service.2,9
Conjunctival nevi are most commonly reported on the bulbar conjunctiva, caruncle or plica semilunaris. They are rarely seen in the fornix, tarsal conjunctiva or within the cornea. However, if the corneal epithelium is involved with a pigmented conjunctival lesion, the possibility of PAM or racial melanosis is higher. Involvement of the cornea by a nevus is unusual, and extension beyond the limbus should raise consideration of conjunctival melanoma.5,9,10,14
Before performing laser photoablation for a conjunctival nevus, the presence of melanoma must be ruled out. The following signs may be associated with melanomas:
-
older patient age when the nevus was first identified
-
corneal, forniceal or palpebral involvement
-
prominent feeder vessels
-
a lack of intrinsic cysts
-
a personal or family history of cutaneous melanoma or dysplastic nevus syndrome.6
Documented growth of the lesion is unusual. In one series of 255 patients, only 4% of individuals showed enlargement.3 In a study from the Moorfields Ocular Oncology Service, nevus growth was reported in 8.5% of patients.9 However, in another study of 410 patients by Shields et al., 180 patients (43%) reported an enlargement of the lesion over time.2 It is interesting that in paediatric patients, despite an increase in size, up to 30% of the nevi may remain amelanotic. This can be diagnostically challenging.10
Slit-lamp examination is required to assess the tumour and the depth of the lesions. Investigations such as anterior segment optical coherence tomography (AS-OCT) are useful in suspicious cases to rule out changes that can occur deep within the lesion. AS-OCT has the ability to identify all margins of the lesion and to rule out any intralesional cysts.15
In the case of large tumours (>4 clock hours limbal tumour or >15 mm basal dimension), an incisional biopsy can be performed before any extensive treatment is undertaken. However, small tumours (≤4 clock hours limbal tumour or ≤15 mm basal dimension) that appear benign on clinical examination can undergo complete resection (excisional biopsy). In certain cases, exfoliative cytology or fine-needle aspiration biopsy can be performed, and useful information regarding the tumour is obtained from just a few cells.11 Ultrasound can also be performed to analyse the depth of the lesion and assess scleral invasion.13
A biopsy is invariably warranted in case a pigmented nevus develops features suggestive of malignant transformation. This can occur in the form of rapid growth, change in shape and/or colour, recurrence after a prior biopsy and unusual locations such as the palpebral conjunctiva or the fornix.10 Malignant transformation is rare. In a study of 410 cases followed up over a mean of 7 years, three patients developed malignant melanoma.2
Conjunctival tumours share the clinical and histological features of mucous membrane tumours. However, the conjunctiva is unique in being exposed to sunlight, unlike other mucous membranes in the body. This could increase the number of melanocytes and cause the occurrence of conjunctival nevi. Sun exposure can also increase the degree of pigmentation and the apparent or actual size of the lesion.7,11,13
Conjunctival nevi show accelerated growth during puberty and pregnancy. This has been attributed to the presence of oestrogen and progesterone hormone receptors in the nevus.7,8 Unfortunately, the distribution of these receptors varies in the literature, raising some doubt about their role in nevus growth. Bredow et al. reported high rates of oestrogen and progesterone receptors in nevus cells.16 However, Pache et al. found progesterone receptors in 96% of samples, but the oestrogen receptors were completely absent in all tumours.17
Management
Most conjunctival nevi are innocuous, without any sight- or life-threatening potential. They can be safely managed by carefully monitoring them, usually on a yearly basis. Anterior segment photographs are useful for record keeping. Shields et al. have mentioned that 43% of their patients claimed enlargement or colour changes of nevi over some years.2 However, photographic evidence proved otherwise, and enlargement was rarely confirmed.2
There are many indications for the removal of conjunctival nevi. They include the ophthalmologists’ concern regarding the transformation of the nevus into a malignant lesion. This is based on lesion growth or enlargement, change in pigmentation and biomicroscopic changes such as an increase in feeder vessels or intrinsic vascularity. The patient may opt for removal of a nevus out of concern for malignancy, ocular surface irritation or for cosmetic reasons.3
The therapeutic options for removal of the conjunctival nevus are commonly argon laser photoablation and surgical excision. Another procedure, the plasma-assisted noninvasive surgery (PANIS), uses atmospheric low-temperature plasma (ALTP) for the ablation of the nevus.14
Laser procedures are reserved for superficial nevi, where there is no possibility of malignancy, or in some specific cases when the patient refuses surgical excision or wishes to try laser ablation first, rather than opting for surgery as the primary procedure.1
Argon laser photoablation is the commonly used laser technique, in which a 532 nm green laser is used. This method has several advantages for the treatment of superficial, benign conjunctival nevi. These advantages include:
-
It is a simple, outdoor procedure that is easy to learn and perform.
-
The procedure is fast, is performed under topical anaesthesia and does not require elaborate equipment to perform.
-
There is complete removal of the nevus with minimal pain.
-
Almost any size of superficial nevi can be managed by this procedure.
-
There are almost no complications following laser photoablation, unlike surgical techniques.5
Among the patients managed by our team, the patients were clinically evaluated for the depth and size of the lesions based on slit-lamp examination. We did not perform OCT or biopsy for any of our patients, as the lesions were primary and were not growing in size to warrant more detailed investigations. Subsequent management was based on whether the lesion was deemed superficial or deep. For superficial lesions, the choice was invariably laser ablation and was successful in all cases. In cases suspected to be deep nevi, the patients were informed about the two management options, i.e. laser and surgical. They each received explanations that laser treatment may not be successful. It was noted that almost half of the patients still preferred to try laser first. However, subsequently, patients had to undergo surgical excision in almost all cases.
In our study, 32 individuals underwent argon laser ablation of the nevi. There are two different protocols mentioned in the literature for argon laser photoablation of conjunctival nevi. In the first, the laser parameters are set at 100-micron spot size, a duration of 0.1 s, and the power is adjusted between 100 and 300 mW. In the other protocol, the laser settings are a 200-micron spot size, a duration of 0.1 s, and the power used is between 300 and 340 mW. We used the first protocol for our patients, as it is less painful and more efficient (Figures 1 and 2).1,5,6
Figure 1: Superficial conjunctival nevus
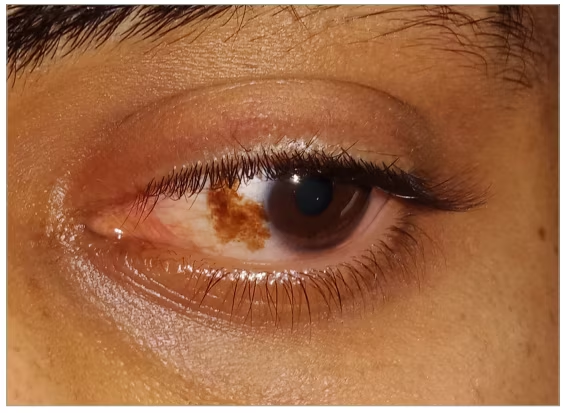
Figure 2: Conjunctival nevus after argon laser ablation

The Pattern Scan Laser (PASCAL) photocoagulation technique is another modification of argon laser ablation of superficial conjunctival nevi. The method involves using a 200-micron spot size, a duration of 0.1–0.2 s and a power of 250–300 mW. Good long-term results with this technique have been reported by Park et al.18
The laser spots are swept over the nevus until the entire lesion is covered by laser marks. The endpoint of the laser setting is the appearance of a burst of pigment, bubble formation, darkening, shrinking or elevation of the lesion.5 Subsequently, the lesion is removed using a cotton-tipped applicator. An antibiotic–steroid eye drop is prescribed for a week, and artificial tear eye drops are prescribed for about 3 months. The patient is advised to use sunglasses whenever exposed to sunlight.
The disadvantages of laser photoablation are a higher prevalence of dry eyes; no specimen is available for histopathological studies; a malignant lesion is completely destroyed without confirmation; and there is a small risk of recurrence.1,5
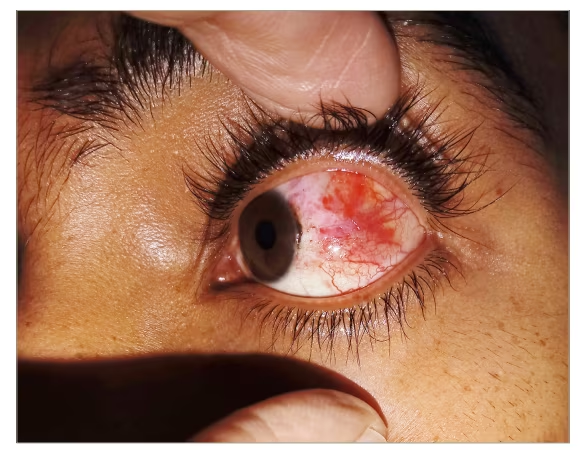
The surgical excision method is usually performed for deep conjunctival nevi. In this study, eight patients underwent surgical excision. A ‘no-touch’ technique is employed to remove the lesion. A local anaesthetic is injected around the nevus. Subsequently, the lesion is excised with a 2–3 mm zone of normal-appearing conjunctiva.10 In cases where the lesion is encroaching upon the limbus, alcohol corneal superficial epitheliectomy is performed. It is recommended to treat the margins of the lesion using the double-freeze–thaw cryotherapy technique.3,10 The edges of the conjunctiva can be sutured together, or, in the case of large defects, amniotic membrane can be transplanted.19,20 In our patients who underwent surgical excision, the sclera was left bare or the edges were sutured with 7/0 vicryl sutures (Figures 3 and 4).
Figure 3: Large, deep conjunctival nevus
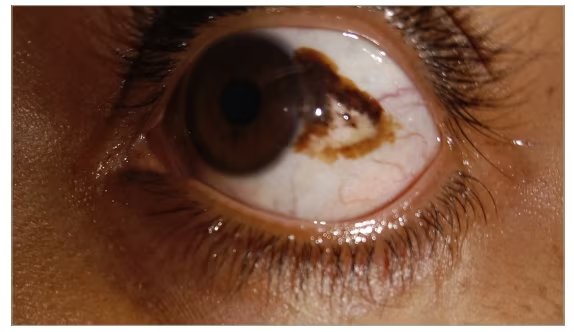
Figure 4: Conjunctival nevus after surgical excision
The advantage of excision is the availability of a biopsy specimen for subsequent histopathological investigation. However, complications can occur, as there is excision of normal conjunctival tissue along with the nevus, leading to inflammation, neovascularization, scarring and tissue dragging.5,6 However, none of these complications were seen in our series of patients.
Conclusion
Conjunctival nevi are the most common benign lesions involving the conjunctiva. They are classified into various types. In most cases, monitoring them is sufficient. There are certain indications where they require removal; in such situations, the therapeutic options are laser or plasma ablation, or surgical excision.
In our experience, the management of conjunctival nevi depends upon the depth of the lesion. Superficial and small lesions can be treated by laser; however, deeper and more extensive nevi require surgical excision. In our series of conjunctival nevi, the results of both procedures were remarkable, and success rates were high in all cases. We recommend proper assessment of the lesions, patient counselling and final management based on these paradigms.











