
On 28 May 2024, enrolment in phase III clinical trials for sozinibercept in neovascular age-related macular degeneration (nAMD) was completed.1 These trials include two large multicentre, double-masked, randomized controlled trials (RCTs): COAST (OPT-302 with aflibercept in neovascular age-related macular degeneration; ClinicalTrials.gov identifier: NCT04757636) and ShORe (OPT-302 with ranibizumab in neovascular age-related macular degeneration; ClinicalTrials.gov identifier: NCT04757610).2,3 These trials represent one of the largest phase III programs in nAMD and are designed to assess the safety and efficacy of sozinibercept in combination with standard-of-care anti-vascular endothelial growth factor (VEGF)-A therapies compared with standard of care alone. The exciting phase IIb results, examining the safety and efficacy of this novel VEGF C/D inhibitor with 366 patients, were published in Ophthalmology in June 2023.4 Given those results, the retina community is eagerly awaiting the primary efficacy 1-year phase III results, which are expected in the middle of 2025.
Photodynamic therapy and pegaptanib
Since the advent of pan VEGF-A inhibition reported in 2005, the conversation has shifted from lines of vision lost to letters of vision gained.5 The previous standard of care was photodynamic therapy (PDT) with verteporphyrin. Using that treatment modality, patients with classic macular neovascularization (MNV) were first studied, and 61% of treated patients lost fewer than three lines of vision compared with 46% of untreated patients at 1 year (p<0.001).6 At 2 years, however, the average visual loss was -11.7 letters in the PDT-treated group and -22 letters in the untreated group.7 Interestingly, for patients with occult or minimally classic MNV, it took 2 years in the PDT group before a significant change in fewer than three lines lost was found: 46.2% of PDT-treated patients versus 33.3% of untreated patients (p<0.023).8 During this era of PDT treatments, inhibition of VEGF isomer 165 with pegaptanib 0.3 mg (FDA approved in December 2004) showed some promise.9 At 1 year, 70% of treated patients lost fewer than three lines of vision, while 33% maintained or gained vision versus 55% of patients in the sham group who lost fewer than three lines of vision and 23% maintained or gained vision.9 This was still better than the natural history of nAMD, where, at baseline, only 20% of patients had vision worse than 20/200, but by 3 years, that had increased to 76% of patients.10
First-generation anti-VEGF agents (ranibizumab, bevacizumab and aflibercept)
Yet with anti-VEGF-A therapy, patients with nAMD had astonishing improvements in visual acuity (VA).5,11,12 Off-label intravitreal bevacizumab saw widespread use starting in 2006, and the FDA-approved intravitreal ranibizumab in June 2006. The ANCHOR (Anti-VEGF antibody for the treatment of predominantly classic choroidal neovascularization in age-related macular degeneration; ClinicalTrials.gov identifier: NCT00061594) trial found a mean VA increase of +11.3 letters with monthly ranibizumab at 1 year, while the MARINA (Minimally classic/occult trial of the anti-VEGF antibody ranibizumab in the treatment of neovascular AMD; ClinicalTrials.gov identifier: NCT00056836) trial found a +7.2 letter increase at 1 year.11,12 In the CATT (Ranibizumab and bevacizumab for neovascular age-related macular degeneration; ClinicalTrials.gov identifier: NCT00593450) trial, ranibizumab and bevacizumab were found to be roughly equivalent.13 At 1 year, VA gain was +8.0 letters for intravitreal bevacizumab and +8.5 letters for ranibizumab.13 Aflibercept was then FDA approved in November 2011, with mean VA increases of between +8.4 and 9.3 ETDRS letters found in the VIEW 1 and 2 (VEGF trap-eye: investigation of efficacy and safety in wet age-related macular degeneration; ClinicalTrials.gov identifiers: NCT00509795 and NCT00637377) studies.14 While aflibercept created some advances with extended dosing intervals, bevacizumab, ranibizumab and aflibercept had roughly similar VA outcomes in most nAMD clinical trials.5,11–15
Second-generation anti-VEGF agents (faricimab and aflibercept 8.0 mg)
The next trend over the last several years has been to look for agents with extended durability. With the newer approved agents, including faricimab-svoa (FDA approved in January 2022) and high-dose aflibercept (FDA approved in August 2023), patients were able to have extended time intervals between treatments while maintaining visual outcomes similar to the previous trials.15,16 Both of these trials were constructed as non-inferiority trials.15,16
The PULSAR (Study of the effects of high dose aflibercept injected into the eye of patients with an age-related disorder that causes loss of vision due to growth of abnormal blood vessels at the back of the eye; ClinicalTrials.gov identifier: NCT04423718) trial for high-dose aflibercept 8.0 mg was compared with 2.0 mg aflibercept with extended time intervals between dosing.15 After three loading doses at 4 weeks, the 2.0 mg group received treatments every 8 weeks, while the 8.0 mg treatment group was divided into 12- and 16-week dosing groups. At 1 year, the 8.0 mg patients in the 12-week group had a +6.7 letter visual gain, while the 16-week group had a +6.2 letter gain. Both of these were non-inferior to the 2.0 mg group, which had a +7.6 letter visual gain.15
Faricimab is a bispecific antibody that targets both VEGF-A and angiopoietin 2 (ang-2). The ang-2 pathway, in pathological conditions, is upregulated and causes increased vascular permeability. With inhibition of ang-2, vessel stability is encouraged. Patients also had extended time intervals of 12 and 16 weeks, which was compared with both 8 weeks of faricimab and 8 weeks of aflibercept. At 48 weeks, in the TENAYA and LUCERNE trials (A study to evaluate the efficacy and safety of faricimab in participants with neovascular age-related macular degeneration; ClinicalTrials.gov identifiers: NCT03823287 and NCT03823300), the faricimab patients, in all treatment intervals, gained between +5.8 and +6.6 letters, respectively.16
Future therapies in the pipeline for neovascular age-related macular degeneration
Current and future studies, including tyrosine kinase inhibitors, gene therapy and other treatment modalities, are also looking to extend treatment durability, but these randomized controlled clinical trials are also constructed as non-inferiority trials for visual outcomes and are typically compared with the current standard of care agents. While the recent and current focus has been on increased durability, physicians have also studied patient preferences regarding better vision, personal cost, on-label indication, treatment intervals and cost to insurance.17 Patients chose VA outcomes overwhelmingly over the other categories (40.4%). It was almost twice as important compared with personal cost (23.1%) and on-label indication (21.3%) and over three times as important compared with a treatment’s durability (12.2%).17 There has been a desire to find other treatment modalities to improve patient’s vision.
Sozinibercept: A novel therapeutic approach
Most of the approved treatments predominantly target VEGF-A, and there has been a ceiling effect over time with these agents. One possible reason for this ceiling effect is that, as VEGF-A is inhibited, VEGF-C and D are further upregulated. VEGF-C and D bind VEGFR-2 and 3, which increase vascular permeability and drive angiogenesis. Sozinibercept (OPT-302; Opthea, Victoria, Australia) specifically targets the inhibition of the VEGF-C and D pathways (Figure 1).4
Figure 1: Members of the vascular endothelial growth factor family and their binding specificity to vascular endothelial growth factor receptors, and the commonly used ophthalmic anti-vascular endothelial growth factor agents4

OPT-302 is a VEGF-C and D ‘trap’ molecule, which sequesters VEGF-C and D and prevents their binding to VEGFRs 2 and 3.
nAMD = neovascular age-related macular degeneration; OPT-302 = sozinibercept; PIGF = placental growth factor; VEGF = vascular endothelial growth factor; VEGFR = vascular endothelial growth factor receptor.
*Bevacizumab is used off-label in nAMD.
Reproduced with permission from Jackson et al. (2023)4
Sozinibercept is a recombinant fusion protein that has a human immunoglobin G1 Fc region fused to a ‘trap’ molecule with binding domains of VEGFR-3, allowing it to bind VEGF-C and D and effectively neutralize them. This prevents ligand binding to VEGFR-2 and 3 and stops the angiogenic effects of VEGF-C and D. This molecule is highly specific only for VEGF-C and D and does not bind VEGF-A, which is why it is used in combination with other anti-VEGF-A agents.
Clinical evaluation of sozinibercept
In the phase IIb study, sozinibercept in combination with ranibizumab was shown to reduce lesion size as well as both intraretinal and subretinal fluid at 6 months.4 Compared with the monotherapy ranibizumab group, the 2.0 mg sozinibercept combination group had a 39% greater reduction in the total lesion area. In the ranibizumab-only group, 29.3% still had subretinal fluid at 6 months, while the 2.0 mg sozinibercept combination group had only 18.5% of patients with subretinal fluid. Similarly, at 6 months, the lowest percentage of patients with intraretinal cysts was in the 2.0 mg combination group when compared with the monotherapy group, 16.8% versus 21.6%, respectively. The average decrease in optical coherence tomography (OCT) central subfield thickness was -146.7 in the sozinibercept group versus -133.8 microns in the monotherapy group (Figure 2).4 No new safety signals were seen in the phase IIb trial and were in line with other large RCT.4 Yet, there is a theoretical risk of increased endophthalmitis incidence with multiple injections, which necessitates increased vigilance (Figure 3).4
Figure 2: Mean change in central subfield thickness4

Mean (± standard error of the mean) change from baseline in spectral-domain OCT central subfield at the predefined 24-week endpoint.
CI = confidence interval; CST = central subfield thickness; OCT = optical coherence tomography; OPT-302 = sozinibercept.
Reproduced with permission from Jackson et al. (2023).4
Figure 3: Safety population analysed according to medication received4
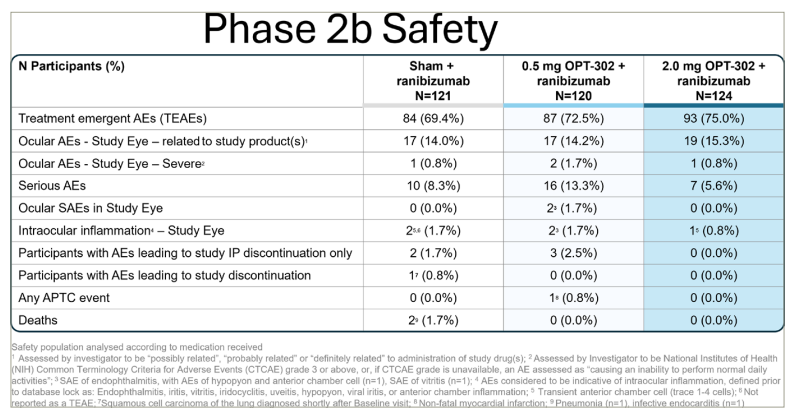
AE = adverse event; APTC = anti-platelet trialists’ collaboration; CTCAE = Common Terminology Criteria for Adverse Events; IP = investigational product; NIH = National Institutes of Health; OPT-302 = sozinibercept; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
1Assessed by investigator to be ‘possibly related’, ‘probably related’ or ‘definitely related’ to administration of study drug(s); 2assessed by investigator to be NIH CTCAE grade 3 or above, or, if CTCAE grade is unavailable, an AE assessed as “causing an inability to perform normal daily activities”; 3SAE of endophthalmitis, with AEs of hypopyon and anterior chamber cell (n=1), SAE of vitritis (n=1); 4AEs considered to be indicative of intraocular inflammation, defined prior to database lock as endophthalmitis, iritis, vitritis, iridocyclitis, uveitis, hypopyon, viral iritis or anterior chamber inflammation; 5transient anterior chamber cell (trace 1–4 cells); 6not reported as a TEAE; 7squamous cell carcinoma of the lung diagnosed shortly after baseline visit; 8non-fatal myocardial infarction; 9pneumonia (n=1) and infective endocarditis (n=1).
Reproduced with permission from Jackson et al. (2023).4
The most exciting and promising aspect of sozinibercept was its statistically significant +3.4 letters gain over standard care (p=0.01). This is almost three lines of visual gain compared with two lines +14.2 letters versus +10.8 letters at 6 months (Figure 4).4 More patients in the 2.0 mg sozinibercept combination group gained ≥15 letters (45.0% versus 40.5%), ≥10 letters (70.0% versus 57.8%) and ≥5 letters (85.0% versus 75.9%) of vision compared with ranibizumab monotherapy (Figure 5).4 Additionally, only 0.8% of patients in the 2.0 mg sozinibercept combination group lost ≥10 letters of vision versus 6.0% in the monotherapy group.4 Also, the study found an 18% relative increase in patients achieving a driving vision of 20/40 or greater compared with ranibizumab alone (Figure 6).
Figure 4: Mean change in best-corrected visual acuity. (± 95% confidence interval) from baseline over time4

BCVA = best corrected visual acuity; OPT-302 = sozinibercept; SEM = scanning electron microscopy.
Reproduced with permission from Jackson et al. (2023).4
Figure 5: Vision gain from baseline to week 24, comparing the percentage gain of those patients gaining ≥5 letters, ≥10 letters and ≥15 letters between OPT-302 and ranibizumab versus ranibizumab only4

OPT-302 = sozinibercept.
Reproduced with permission from Jackson et al. (2023).4
Figure 6: Percentage of patients with 20/40 vision at week 24

Opthea data on file.
OPT-302 = sozinibercept.
Future perspectives
With both COAST and ShORe fully enrolled with almost 2,000 patients, we are eagerly awaiting the 1-year primary efficacy endpoint results to see if these large RCTs will again demonstrate superior vision gain. We will see if we can raise the ceiling for our patients by improving visual outcomes using this new therapy in combination with our other approved standard-of-care therapies. With sozinibercept representing the only late-stage therapy targeting superior vision above and beyond current therapies, many more of our patients will likely see better visual outcomes.










