Whether bi-manual or co-axial, the microincision phacoemulsification techniques of today allow for a neutral cylinder, thus reducing high-degree aberrations (in particular the coma type). The hydrophilic acrylic intraocular lenses (IOLs) are more compliant as they are inserted through a minimum 1.6–1.8mm incision, whereas the hydrophobic IOLs are inserted through 2–2.2mm incisions but generate fewer secondary cataracts. The general idea of aspherical IOLs is to compensate all or part of Z4 types of positive corneal spherical aberrations (SAs) with a properly adapted optic. On average, corneal spherical aberrations are +27μm for a 6mm pupil, which corresponds to a mean Q co-efficient of -27. In order to choose the correct asphericity profile, the patient’s corneal profile must first be studied by measuring not only the Z4 and Q factor but also his/her keratometry data. It is necessary to know the levels of asphericity of the different IOLs on the market and finally to take into consideration the power of the implant.
Current corneal topographic devices measure the value of the Q factor directly, as well as the spherical distortions of each cornea. Historically, the first implants totally compensated corneal SAs, but over the last few years we have been aiming at only partial correction of these SAs in order to achieve the best visual result, which we know is obtained with approximately +0.10μm total residual SA.1 As correction of SAs also provides a better contrast sensitivity in photopic and mesopic conditions, the main clinical interest in correcting spherical SAs is specifically seen in mesopic and scotopic conditions with a pupil dilated at approximately 6mm, which improves the ability of night driving. With this in mind, it can be interesting to systematically carry out corneal topography on all young patients having undergone cataract surgery in order to optimise their vision in these conditions,2 because we know they will be driving at night. On the other hand, depth of focus induced by implants correcting SAs can be reduced, but this is not an established fact as different studies have sometimes given conflicting results.
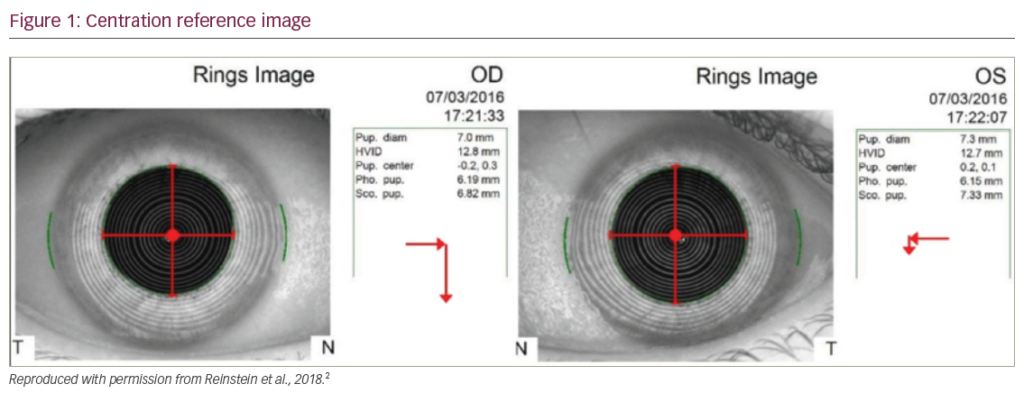
The results of a prospective multicentre study carried out by four surgeons concerning a microincision implant (see Figure 1) offering a -0.11μm asphericity through a 1.8mm incision (Micro AY implant made by PhySIOL laboratories) are presented here, covering 124 cases of senile or pre-senile cataracts. The population was made up of 54% females and 46% males, of whom 23% presented cortical type of cataract, 58% nuclear cataracts and 19% subcapsular cataracts. Mean age was 73.5±8.3 years (range 51–89 years). Topical anaesthesia was used in 96% of cases with 100% clear cornea incisions. The incision was temporal in 59% of cases, 27% on the most arched meridian and superior in 3% of cases. The bi-manual technique was used for 92 (74.2%) of patients. The mean incision for phacoemulsification was 1.41mm for all of the interventions and 1.95mm for implantation.
Mean endothelial cell loss was 6%. Of 101 cases, uncorrected visual acuity was 0.72±0.22 at three months and best corrected visual acuity (BCVA) was 0.97±0.25 (see Figure 2). Post-operative spherical equivalent was -0.36±078D (compared with 0.51±2.31D preoperatively). Pre-operative cylinder was -0.34±0.87 and reached -0.14±0.71D post-operatively. In aberrometry, the pre-operative corneal Z4 were +0.24±0.13 (from -0.09 to +0.31) and reached +0.10±0.11μm (from -0.12 to +0.24) post-operatively. No complications were due to the implant: there were no problems during insertion with the PhysIOL injector, no decentration, no IOL deposits and no posterior capsule early opacity (see Figure 3). Results for contrast sensitivity are presented in Figure 4; depth of focus (DF) was compared with a series of spherical lenses, confirming that there was a slight decrease of DF (see Figure 5) but to a lesser extent than in full correcting SA IOLs.
This study confirmed that the refractive approach to SAs of the cataract improved the pseudophakic’s quality of vision. On the whole, customising the correction of SAs will depend on the corneal topography in certain cases: young adults driving at night, patients with large pupils, those with diffractive multifocal IOLs and patients with particular corneal profiles, especially those having undergone refractive surgery. Indeed, it has been pointed out that a mean partial correction of SAs in all of the studies shows an increase in contrast sensitivity with implants having an aspherical optic as long as the implant is correctly centred. However, correcting spherical aberrations will always come after the correction of spherical and cylindrical ametropia relevant to the quality of surgery and the precision of biometrical calculations.