Femtosecond lasers (fs-lasers) have developed rapidly, and several approved laser systems are on the market. The spectrum of applications has also expanded considerably. In corneal surgery, the precise intrastromal use of the fs-laser has opened numerous new applications and led to totally new surgical standards. The fs-laser is an infrared laser that functions with much less heat stress than other laser systems. Its use enables surgeons to separate corneal tissue precisely without a scalpel. The tissue should be largely transparent so that the laser can make precise incisions at any site on the cornea. At the clinic for refractive and ophthalmic surgery in Duisburg, Germany, we use a modern 40khz version of the Femtec fs-Laser (20/10 Perfect Vision, Heidelberg, Germany). When using the fs-lasers now available on the market, the cornea is subjected to applanation, leading to vision blackouts during treatment. The Femtec fs-laser has a patented, curved patient interface. Thanks to the curvature, only moderate suction is needed to couple the eye to the laser. The treatment itself is performed with minimal applanation and therefore without vision blackouts during the surgeries. The procedures performed are endothelium-sparing. In our opinion, there are two approaches to future applications of fs-lasers. One is to survey the present practical applications closely and further improve and develop existing surgical techniques. We will start with this approach and illustrate it with case studies. The second approach entails examining current research for which concrete scientific publications are available. However, it must be questioned to what extent the, admittedly very attractive, approaches can be applied in practice and when – if ever – this will be the case. This preview will conclude our overview.
Flap Preparation
Laser-assisted in situ keratomileusis (LASIK) flap preparation in refractive corneal surgery was the first application in which we used the fs-
laser.1 Compared with mechanical microkeratomes, using the fs-laser resulted in greater precision at the intended flap depth with considerably less standard deviation.2,3 Another advantage is the possibility of fitting the flap individually to the corresponding LASIK, i.e. the hinge position, flap diameter and thickness can be selected as required. Use of the fs-laser is especially advantageous in thin corneas. We can also make safer laser cuts in cases of greater astigmatisms since the cornea is flattened to about 35 diopter (D). The laser cut is made under complete visual control and can be terminated if necessary. The following case illustrates our procedure.After cararact surgery, the 68-year-old patient had refraction of +1.0–4.0/35º=0.63. Pachymetry measured 569μm at the thinnest place. We selected a diameter of 8.5mm with superior hinge position, a flap thickness of 140μm and an angle of 90º as parameters for flap preparation. The procedure took only 45 seconds.
The precise angle in particular facilitated repositioning the flap. One day post-operatively, vision was identical to the pre-operative value, with an astigmatism reduction to 3.5D. Four weeks post-operatively, the astigmatism was 3.25D. We observed that less tissue had to be removed in patients with greater astigmatism in a double surgery, since tension can be reduced in the cornea only by the flap preparation. As soon as the value was stable, we performed the LASIK in a second session. After LASIK, the patient had refraction of -0.25=0.80 immediately post-operatively. This value remained stable four months post-operatively. We now perform Femto- LASIK routinely in Duisburg. We consider the greater precision in flap preparation and the possibility of individualised procedures to be clear advantages. We will see further development of this application in using oval flap forms in astigmatisms in the future. In addition, as in lamellar keratoplasties (KPL), an intrastromal pouch can be created in which the intracorneal inlays can be reversibly implanted.
Astigmatic Keratotomy Incisions
The surgeon can select the length, site, depth and position of the incision(s) at will. The fs-laser guarantees greater precision and reproducibility of incision, for example in greater astigmatisms in penetrating keratoplasties (pKPLs).
Treatment of Progressive Keratoconus with Implantation of Intracorneal Ring Segments
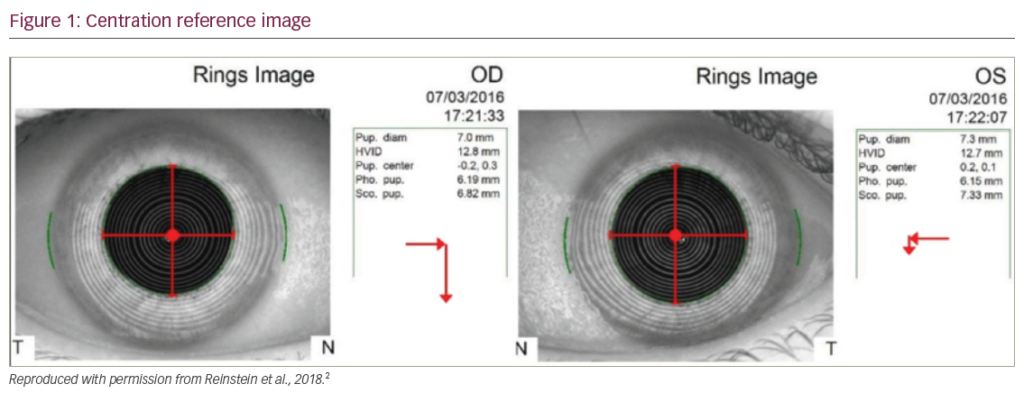
Since December 2004, we have successfully been treating patients with progressive keratoconus (with clear central cornea4–7) by implanting intracorneal ring segments (ICRS), e.g. Intacs™.8–11 We use the fs-laser to prepare the implantation tunnel. This enables us to make intrastromal preparation from interior to exterior at 70% corneal depth. We prepare a tunnel of exactly 1mm. Depending on the patient’s individual findings, we set the outer diameter between 8.0 and 8.8mm and the inner diameter between 7.0 and 7.8mm. In less than one minute, we have a minimal implantation tunnel that can be adapted in form and size to the patient. The ICRS are implanted using instruments specifically designed for the purpose, whereby hardly any space is left between the implantation tunnel and the ICRS. The cases cited of an ex- and re-implantation12,13 of ICRS illustrate the precision of the surgery if an fs-laser is used. In another clinic, ICRS were implanted in a right eye with an incorrect axis position. The cornea of the 42-year-old woman with bilateral keratoconus steepened additionally (see Figures 1 and 2). Neither glasses nor fitting of contact lenses was possible. Myopia and astigmatism increased after the surgery.
Our measurements revealed that the ICRS were implanted at a peripheral depth of 417μm. Pachymetry showed that the thinnest point in the cornea was in the conus, with an area of 384μm corneal thickness. Vision was -6–11/85º=0.2. We decided to explant the ICRS. After a two-week healing phase in which the epithelium stabilised, the corneal astigmatism was 9.1D. Best corrected visual acuity (BCVA) was -8.25–9.0/60º=0.2 (see Figures 3–5). Since the depth of the old implantation tunnel was 417μm, we prepared the new tunnel intrastromally using the fs-laser at exactly 350μm corneal depth, with a width of 1mm and an outer diameter of 8.8mm; the ICRS were then implanted at a shift of exactly 90º. At the first post-operative day, uncorrected visual acuity (UCVA) was 0.63 and the astigmatism was -2.2D. Three months post-operatively, UCVA increased to -1.5–3.5/25º=0.8. The patient was fitted with a miniscleral lens with a diameter of 11.2mm and strength +1.37 to correct the remaining visual deficit. BCVA was 0.8–1.0p. This value remained stable even six months post-operatively, and vision remained good and unchanged. There was no further steepening of the cornea. We have now treated more than 78 patients and have a post-operative period of more than 2.5 years. In nearly all patients, we found significantly flattened and shifted conus, stable ICRS, clearly reduced astigmatism and significantly improved BCVA of more than 50%. None of the patients has required pKPL. As a consequence of the versatile fs-laser cuts, individual ICRS will undoubtedly be available in the near future.
Penetrating and Lamellar Keratoplasties
We performed our first pKPLs with the fs-laser in 2005 with very promising post-operative results. In preparing the donor cornea, we begin the laser cut at a depth of up to 1,200μm and continue this up towards the epithelium, which is very endothelium-sparing. We always select a 90º cutting angle to the corneal curvature. Thanks to high laser precision we can select identical diameters and cutting angles for both donor and recipient corneas. Preparation of the recipient cornea is just as precise, whereby pressure to the bulbus during the procedure is only ~35mmHg. Again, we begin the laser cut at a depth of up to 1,200μm and continue it up towards the epithelium. After the recipient cornea has been removed, the prepared donor cornea nestles perfectly in the opened eye. The extremely precise cutting angles allow the corneal tissues to fit almost exactly into one another. We start with four-point suture for fixation before making the continuous sutures. Visual control is maintained during the entire preparation. The eye remains a closed – and thus a stable – system for as long as possible during surgery. Preparation is considerably quicker than with the usual methods. We have now performed more than 30 pKPLs with the fs-laser and have a post-operative observation period of up to 22 months. All patients had stable anterior chambers and well-adapted, clear transplants without post-operative folds. We noticed a marked improvement in vision and more rapid wound healing. Thus, based on our experience, we can confirm the advantages of pKPL with the fs-laser reported in publications.14,15
In November 2005, we performed our first anterior lamellar KPL. The 72-year-old patient had paracentral corneal scars with indentations in the central edge area and corneal vascularisations. Pre-operative vision was +8.0–3.75/35º=0.05. Corneal pachymetry showed 384μm at the thinnest part. We began with the preparation of the donor cornea, selecting a diameter of 9.1mm, a thickness of 230μm and a cutting angle of 90º. Intrastromal preparation was made from the epithelial side. We selected the same diameter (9.1mm) and cutting angle (exactly 90º) for preparation of the recipient cornea. A slightly lower trepanation thickness of the donor cornea of 200μm was selected. The preparation was again made intrastromally from the epithelial side.
The prepared donor cornea fits almost perfectly in the recipient tissue and can be sutured without problems. A therapeutic contact lens was then applied. Post-operatively, the patient showed excellent, rapid wound healing. The cornea was well-adapted, clear and without folds. Five days post-operatively, BCVA was +0.75–2.25/70°=0.4. Four months postoperatively, BCVA was +2.00–3.75/85°=0.4, and remained unchanged.
This surgery is considerably less traumatic and more precise when using the fs-laser compared with a mechanical procedure. There is visual control during the entire procedure. The surgeon can individually select the diameter of the transplants and the cutting angle. The KPL can be adapted to the patient’s particular disease. We now routinely perform pKPLs and lamellar keratoplasties with the fs-laser. Experience to date shows that these procedures are safe, precise and effective. A new operating standard is set for both procedures with the use of the fs-laser. A variety of transplant forms16,17 are plausible in future development in addition to the standard incision, for example decagonal form, hexagonal form, top hat, mushroom, zigzag, Christmas tree and zig square. It remains to be seen which transplant form will be optimal in the long run.
Endothelial Keratoplasty
A further possible application is fs-laser-assisted lamellar endothelial keratoplasty (FLEK).18 We began preparation with the donor cornea in the artificial anterior chamber. Starting from the endothelial side, we made a straight intrastromal laser cut with a 90° cutting angle to the desired corneal depth. The circular laser cut was continued intrastromally to a pre-defined depth of, for example, 120μm and a pre-defined diameter of ≥6mm. After completion of the laser procedure, we turned the donor cornea over and prepared the back with a flat spatula. During preparation of the recipient cornea, the patient’s eye remained a closed system until the actual transplant exchange. The recipient cornea was prepared with identical parameters (diameter, incision depth and cutting angle) as the donor cornea. We began again with an intrastromal endothelial straight laser cut with a 90° cutting angle (sharp edge). The laser cut was continued to a depth of 120μm, then a circular lamellar cut was again made with the pre-defined diameter.
Our first endothelial transplantation was made through a 3mm clear cornea tunnel. First, the endothelial layer was separated with a spatula and removed. The endothelial layer of the donor cornea was folded, implanted and positioned through the paracenteses using instruments and viscoelastics. As soon as the procedure had been completed, air was suffused into the anterior chamber as post-operative tamponade. Due to the narrow indication, we have performed this procedure in only a few patients, and have only four-month post-operative results thus far. The patients show clear corneas and stable BCVA. The main advantage of FLEK is the possibility of performing the procedure intrastromally with pre-defined depth, cutting angle and diameter. Thanks to the exact cutting angle preparation, the risk of postoperative decentration is minimised. In any case, we will continue FLEK and refine the surgical technique.
Preview of Future Uses
With respect to future possible uses of the fs-laser, available reports indicate preliminary research approaches that are still in the experimental phase, rather than concrete perfected applications for use in patients. One major objective of fs-laser use is direct intrastomal (lamellar) vision correction without opening the eye, especially hyperopia and presbyopia correction. Treatment of presbyopia is addressed by the attempt at phakic operative lens treatment, whereby it is necessary to wait and see how the natural human lens changes over time due to the intervention. Blum et al.19 report that incisions could be created in both animal experiments and human lenses that increase the elasticity of the lens. The team demands more complex eye models and further development of diagnostic instruments for characterisation of levels of presbyopia and objective evaluation of later therapy success for future non-invasive presbyopia treatment. Gerten et al.20 reported on lentotomy in treatment of presbyopia performed with ultrashort fs-laser impulses. An fs-laser lentotomy was performed in vitro on 150 porcine eyes to gather experience with incision geometry and optimal laser settings for minimal formation of gas bubbles. In vivo, four rabbit eyes were treated and observed up to three months post-operatively. The lenses were then explanted and examined. Important parameters could be identified to create smooth, precise incisions. No cataracts formed during the follow-up period. Krueger et al. attained comparable results in 2005.21 This team also worked with fs-laser modulations of animal lenses and on the possible formation of cataracts. They reported that laser modulation of the lens did not show any influence on lens function up to three months post-operatively, and no cataract formed during this time. They concluded that low-energy fs-lasers can be used safely for modification of the lens as treatment of presbyopia. Another interesting approach is the use of the fs-lasers for glaucoma treatment (glaucoma surgery). We must point out that the use of the fs-laser has concentrated thus far on transparent corneal tissue. Whether the same precision can be achieved with less transparent tissue remains to be seen. Toyran et al.22 examined the use of the fs-laser on human trabecula meshwork in an in vitro study. They concluded that “…with appropriate exposure time and pulse energy, fsec (femtosecond) photodisruption can be employed to create lesions in the human trabecular meshwork without damaging the surrounding tissues. This study demonstrates that fsec laser treatments may have future potential for the surgical treatment of glaucoma.” Ngoi et al.23 carried out an in vitro study to determine whether less ablation energy can be applied using the fs-laser compared with lasers with longer pulses; this was confirmed. In 2002 and 2003, Sacks et al.24,25 examined the precision of subsurface photodisruption in translucent sclera. They reported that posterior scleral photodisruptions could be performed in vitro with high precision for a number of intrascleral incisions.
Conclusion
The use of the fs-laser in corneal surgery led to important novel approaches and completely new surgical standards. More recent applications, such as hyperopia correction, presbyopia correction by lentotomy or the possible treatment of glaucoma with an fs-laser, only hint at the enormous potential of this fascinating technology.